How is it that the nation we live in is a powerhouse economy, yet we rank 43rd in life expectancy in the world?What are we doing wrong and what can be done to change this? An issue we are facing is that we are simultaneously dealing a health crisis and political crisis. The health care system and our response to a pandemic is exacerbating the governmental and political climate in relation to health policy. Our nation is empowered and driven by wealth, thus if individuals don’t have the economic stability, they won’t be able to combat the health disparities that come with it. This is a problem because we are not valuing citizens, we are valuing business and the capitalistic society that surrounds us. We live in the United States of America; however, we are not anywhere close to what a united country should look like, and frankly, might never be. Globally, the health of individuals is the main topic right now. Viruses and their relation to health are currently having a strong influence on the actions each person takes whether it be with school, work, or daily errands. I am here to argue that there are disparities seen in minority and low-income populations across many health outcomes and this is due to the lack of security we have with our education and health system. I am not advocating for universal health care; however, I am arguing that health care should be seen as a right, not a privilege. We should create a space within communities and education systems to promote health care as a right and make resources more available to those in need.
We are, above all, entitled to our freedoms. However, this liberty is being challenged by the many different factors that make up our society. Although a powerhouse house country, disenfranchised individuals are still being affected by the social and economic factors that affect our health outcomes. This is a battle that not everyone faces, but it is prevalent amongst many communities across the nation and even across the globe. It is made aware to me that people are not aware of the health disparities that are being exacerbated by the coronavirus pandemic. In a recent news article the issue being presented surrounded the disparity seen amongst individuals living in New York (Pilkington and Ankita). This article discusses how the coronavirus has created two societies that are divided by socioeconomic status and race. The divide is seen to reflect the data of death rates and death figures in New York (Pilkington and Ankita). The author states, “Coronavirus may not discriminate but the outcomes do” (Pilkington and Ankita). This means that the outcomes of the disease are having different burdens based on other factors aside from the disease itself. The coronavirus is a threat to everyone; however, some people are more capable of practicing health promoting behaviors, like social distancing, buying healthy food at the market, or working out in their backyard. This is not the case for everyone in the United States and also around the world. Some people are still struggling to put food and water on the table, some are still rushing to work essential jobs, and some have underlying conditions associated with poverty and racism. These factors are all contributing to vulnerability to the disease and the related outcomes. This article highlights how health is seen as a privilege. It is inevitable that there will be social differences throughout our country, but this doesn’t mean that health inequities should coexist with social inequities.
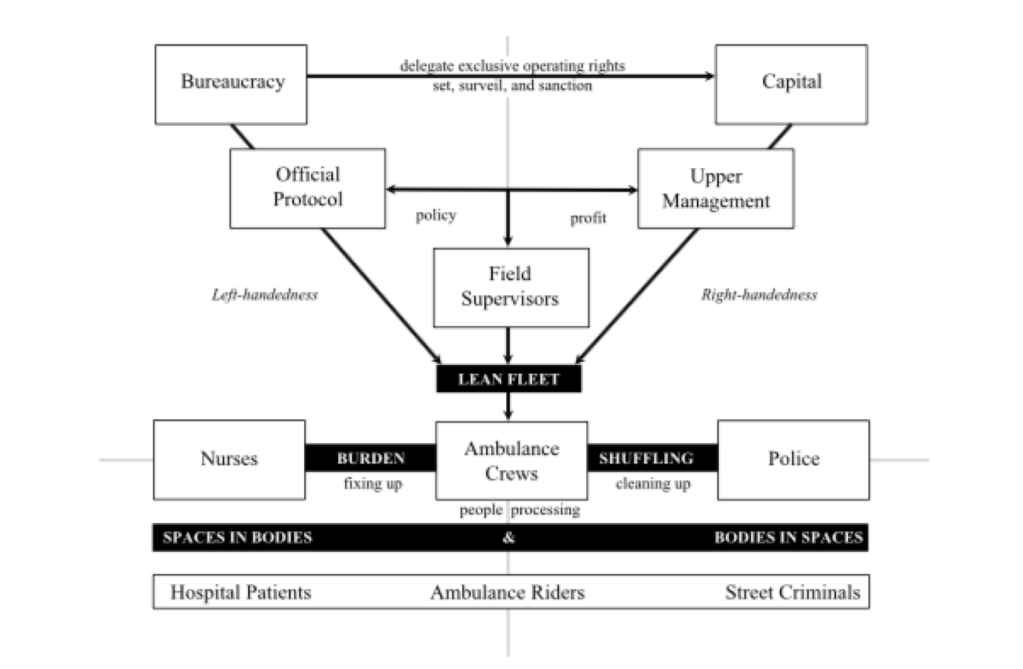
The health disparities seen throughout our country are explained in detail with an article about burden shuffling with ambulances and hospitals (Seim). The bureaucracy and capital are composed of upper management and supervisors that drive profit and create policies while the nurses, ambulance crews, and police are shuffling between fixing up patients and getting patients off the streets (Seim 460). This article explains how America’s sick-role is a part of a multi-dimensional process where poverty, disease, and deviance are seen as form of social control. This article shines the light on the disparities we see with health care based on socioeconomic status. There are horizontal and vertical components that work together to affect each other and the labor processes related to health and deviance. We are operating spaces in bodies and bodies in spaces. Spaces in bodies; where we treat individuals and their physical structure, and bodies in spaces; where we are, for example, moving a psych patient off the streets to protect others (Seim 452). Poverty governance is a social determinant and theory that is associated with our health care system. We need to create a different approach to change health care policy and profit. This can be done by taking action within the community to advocate for change in health education and promote awareness for those who lack the knowledge.
Health disparities across the nation are guided by an individual’s educational attainment. As an undergraduate student, I already have more leverage to have better health outcomes than others who aren’t receiving higher education. In a study done by Stanford University colleagues, data from the 2012 Medical Expenditure Panel Survey was used to measure physical health status, educational attainment, sociodemographic variables, and the access to or use of medical care (Kaplan). Their results of the average physical component score for both men and women were highest with those with graduate and bachelor degrees (Kaplan). This suggests that there is a systematic relationship between educational attainment and self-reported physical health scores (Kaplan). Overall, the access and use of health care is a direct reflection on the health-education gradient explained in the article. This is why it’s important to encourage a quality education because this can outweigh other social determinants in terms of promoting better health outcomes. In order to bridge the gap between low-income communities and health care, I think it’s important that we work closely with education systems and universities on health promoting behaviors that people can practice. The advice doctors provide to patients should be made aware to everyone.
To address the related health disparities in our country, we must address restructuring the education system. There are so many different situations in which we can make an impact to influence policy makers and the macro level structures. Advocating for health education programs creates and space for students of all levels to develop an understanding of health outcomes and educational attainment. Implementing health education into the education system brings more awareness to the social determinants relating to health. Creating places for students to learn more about how they can contribute to better health behaviors for themselves, also promotes student’s interactions in helping their families and the community they live in. Another far-stretched idea that could drastically change health disparities are offering medical resources to students and their families. Some students in both privileged and impoverished areas, look forward to school because it is their safe haven. If we could make this a place for students to be educated about their health as well, we could further reduce these health disparities and change the tide of health outcomes for future generations.
With an understanding that there may be constraints to do the governmental role in health care, I still think it is most important for health care workers to address the health disparities seen in minority and low-income populations. The ones who have a voice in health care policy aren’t always the ones who have had the hands-on exposure. This is why I believe healthcare workers should have more of a stance in health policy. So often we focus on the political climate with decision making rather than the facts and science that could benefit communities. As a society, it is important that health care professionals and medical experts advocate for the health of people rather than patients. Instead of treating each individual as a number, we need to treat each individual as a value to society. Overall, I think we all deserve an equal chance to maintain a healthy lifestyle and have the resources to do so. Even if these resources provide the minimum for low-income and disenfranchised communities, it is better than what we offer now.
Works Cited
Kaplan, Robert M., et al. “Educational Attainment and Health Outcomes: Data from the Medical Expenditures Panel Survey.” Health Psychology, vol. 36, no. 6, 2017, pp. 598–608., doi:10.1037/hea0000431.
Pilkington, Ed, and Ankita Rao. “A Tale of Two New Yorks: Pandemic Lays Bare a City’s Shocking Inequities.” The Guardian, Guardian News and Media, 10 Apr. 2020, http://www.theguardian.com/us-news/2020/apr/10/new-york-coronavirus-inequality-divide-two-cities.
Seim, Josh. “The Ambulance: Toward a Labor Theory of Poverty Governance.” American Sociological Review, vol. 82, no. 3, Apr. 2017, pp. 451–475., doi:10.1177/0003122417702367.
